Public awareness and practices towards health impacts of PM2.5 in the Kingdom of Bahrain: identifying areas for intervention
Article information

Abstract
Air quality has critical public health impacts as several diseases have been attributed to exposure to high PM2.5 concentrations. In the Kingdom of Bahrain context, while the sources of PM2.5 and prevailing trends have been studied, its social and health dimensions remain a gap in the literature. This study explores public perceptions of PM2.5 in the Kingdom of Bahrain, focusing especially on public awareness of PM2.5, its sources, and its health impacts. It further highlights actions taken by individuals to mitigate associated health impacts. This cross sectional study was based on the Driver-Pressure-State-Impact-Response framework. A self-administered questionnaire was distributed to the public, a total sample size of 263 responses. Descriptive statistics, including frequencies and percentages of participants’ responses, were calculated. The Independent Samples t-test and a one-way analysis of variance (ANOVA) were applied along with the Chi-Square test to identify factors associated with the public’s knowledge and practices relating to PM2.5 in Bahrain. A p-value of less than 0.05 was considered as statistically significant. A significant proportion of the participants were unaware of PM2.5, its concentration in Bahrain, and whether it is being measured. However, the majority of respondents had respiratory problems and took self-protective measures when the air quality was bad. There were statistically significant differences in the adoption of precautionary measures, which was prevalent among participants suffering from respiratory problems. Around 32% of the respondents were willing to pay monthly contributions to improve air quality and indicated their interest in receiving information on Bahrain’s air quality via social and mass media. The findings suggest that there is a need to raise public awareness towards air pollution and its health effects. Moreover, epidemiological studies should be conducted to advance understanding on how air pollution is linked to morbidity and mortality in Bahrain.
Introduction
Environmental health is a key component of public health. According to the World Health Organization (WHO), around 13.6 million deaths (24% of the total number of deaths globally) were attributed to environmental factors, with 25% of these deaths directly linked to exposure to fine particulate matter or PM2.5 [1]. Exposure to ambient PM2.5 is a causal factor in the following diseases: lower respiratory infections, lung cancer, chronic obstructive pulmonary disease, stroke, ischemic heart disease, and type 2 diabetes [2].
A study on the Global Burden of Disease (GBD) led by the Institute for Health Metrics and Evaluation at the University of Washington (IHME) that commenced in 1990 estimated cause-specific mortality at the global level. Its findings constitute the basis of many studies that have examined the causes of injuries, diseases, and risk factors. In October 2020, the updated findings of the GBD study were published [3].
Although the results of the original GBD study have been utilized in many studies, few of these studies were about diseases attributable to PM2.5 and none of them investigated PM2.5-related deaths in the Gulf Cooperation Council (GCC) countries, namely Bahrain, Saudi Arabia, Kuwait, Oman, United Arab Emirates and Qatar. The literature on PM2.5 in the GCC countries ranges in geographical scope from the national level to regional and international levels and focuses on the physical and chemical characteristics of PM2.5, its sources, trends, and health consequences. Most of the studies within this body of literature were published from 2015 onward, with a very small proportion examining the health effects of PM2.5. Studies on PM2.5 in Bahrain have mainly focused on the temporal and spatial distribution and sources of PM2.5 and prevailing trends [4–6]. Only one study indirectly examined its health-related effects by linking air quality with seasonal variations in consultations relating to several diseases, including respiratory diseases. However, no direct link was posited between the PM2.5 concentration and morbidity or mortality in Bahrain in this study [7].
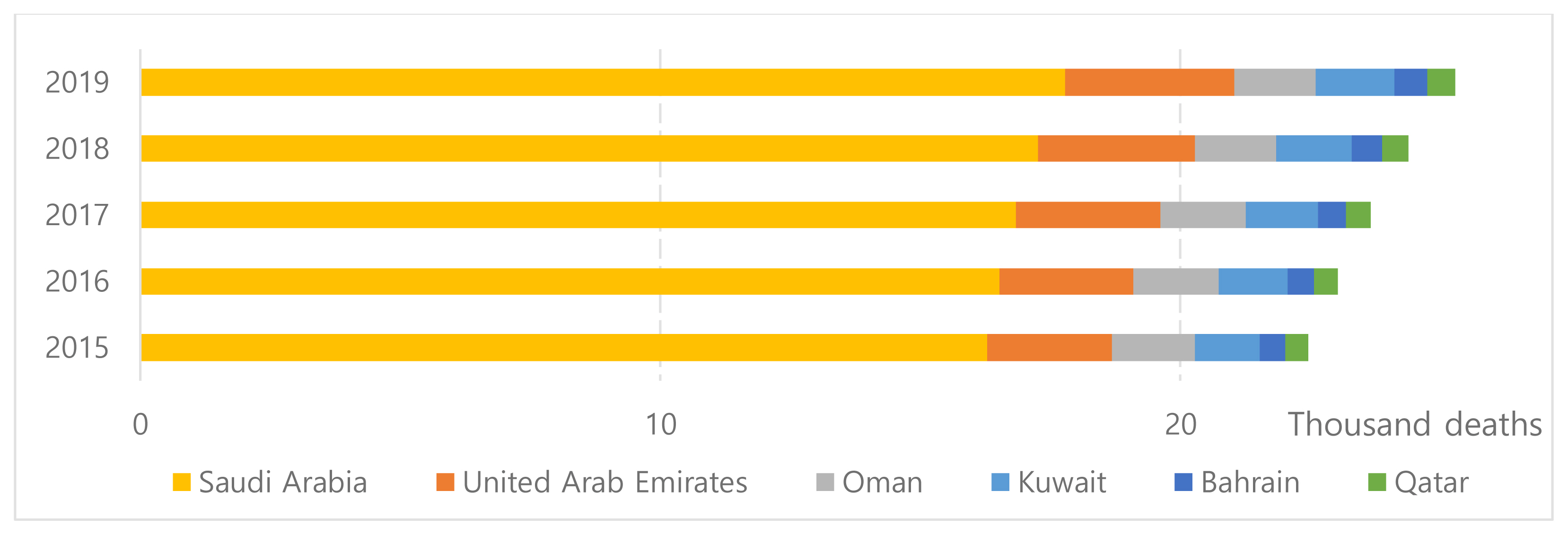
Ambient air pollution is a serious environmental issue in the GCC countries. The global rankings of all the GCC countries in relation to their PM2.5 concentrations are 140 or higher in the Environmental Performance Index [8]. In 2017, the mean annual concentration of PM2.5 in all of these countries to which their entire populations were exposed ranged between 53 μg/m3 (in Oman) and 107 μg/m3 (in Qatar) as reported by The World Bank [9]. These figures evidence increased PM2.5 concentrations compared with levels in 2015, when the minimum and maximum concentrations were 35 μg/m3 and 80 μg/m3 in Oman and the United Arab Emirates, respectively [10]. The PM2.5 concentrations in these countries, which exceed the WHO’s recommended standard of an annual mean PM2.5 concentration of 5 μg/m3 [12], could be responsible for deaths in the GCC countries that increased from 22,400 in 2015 to 25,200 in 2019 (Figure 1) [13]. Vehicles and electricity generation have been identified as the key sources of PM2.5 in Bahrain, Kuwait, and Qatar [14].
Many of the GCC countries have devised strategies to improve air quality and have set standards for air pollutants to reduce the health and environmental-related impacts of PM2.5. The adoption of various forms of renewable energy and a shift to public transport are also evident in these countries. The Arab Strategy on Health and the Environment 2017–2030, introduced by the Arab League, covers nine priority areas that include air quality and especially particulate matter. Several strategic objectives relating to air quality, including raising public awareness and taking actions to reduce air pollutants at the source, are proposed in this strategy [15]. However, the public’s role as users of air and contributors to air quality improvements remains largely unexplored in countries across the globe, more generally [16], and in the GCC countries in particular. There is a growing body of international literature on public awareness, attitudes, and behaviors regarding PM2.5. For example, in one study, members of the public were involved in the data collection process that entailed taking readings of particulate matter, thereby raising their awareness and advancing their understanding regarding this issue [17]. Another study suggested the need to align China’s Action Plan on prevention and control of air pollution with public perceptions of the risks posed by PM2.5 [18]. Other studies in the Chinese context have investigated the public’s willingness to pay to improve air quality [19,20].
Yet, in the case of the GCC countries where the annual mean values of PM2.5 concentrations exceed the WHO’s recommended standard, published studies on public perceptions regarding this issue are lacking. A survey regarding air quality in Bahrain was conducted on 150 participants with emphasis on PM2.5, however it was lacking the factors affecting the knowledge and practices of the public towards it [21]. Thus, there is a critical need for a study that explores public knowledge and practices and provides vital inputs that contribute to maintaining good health and reducing air pollution.
By examining public perceptions of PM2.5 in the Kingdom of Bahrain, which is one of the GCC countries that is characterized by a relatively high annual mean PM2.5 concentration, this study will contribute to addressing the above knowledge gap by exploring public awareness in the Kingdom of Bahrain about the sources of PM2.5 and its health impacts, identifying practices and measures adopted by the public to mitigate the health impacts of a relatively high concentration of PM2.5, and examining factors associated with knowledge and practices of the public towards PM2.5.
Materials and Methods
This cross sectional study entailed a quantitative approach to data collection and analysis. The instrument was a self-administered questionnaire that was distributed to the public in Bahrain, which has a total population of approximately 1.5 million, of whom 52% are expatriates according to the Information and e-Government Authority [22].
Questionnaire design and distribution
The questionnaire applied in [21] was modified and used in this study. It was designed and developed with reference to the literature [17,23,24] and according to the Driver-Pressure-State-Impact-Response (DPSIR) framework to achieve the study’s objectives [21]. This questionnaire has been used in this study with the modification of the 5-point Likert scale for the responses into a 3-point scale. The DPSIR framework is widely used in environmental studies and has also been applied in studies focusing on the health-environment interface [25]. The questionnaire comprised three sections: participants’ information and consent, demographic items, and items on knowledge and practice. The third section was divided into two subsections. The first subsection measured respondents’ knowledge about PM2.5, its sources, impacts, and government responses. The second section focused on practices and mitigation measures adopted by the public. The questionnaire entailed a mixture of open-ended and closed-ended questions. The majority of closed-ended questions required “yes”/”no”/”do not know” responses, and there were several multiple-choice questions.
An online questionnaire was developed via Google Forms. A convenience sampling strategy was applied, and the link to the questionnaire was shared via WhatsApp and emails inviting participants, who voluntarily participated. No IP addresses were saved, and incomplete surveys that were not formally submitted were not recorded to ensure the participants’ anonymity.
A pilot study was initially conducted with 20 participants. Several questions were revised based on comments received from these participants. Two versions of the questionnaire in Arabic and English were prepared and distributed to Bahraini nationals and non-nationals. There were two participation criteria: the respondents were 18 years and above and agreed to participate. No monetary or non-monetary incentives were offered to participants. The questionnaire was distributed to more than 500 participants, and 263 valid forms were received.
The questionnaire applied in [21] was modified and used in this study. It was designed and developed with reference to the literature [17,23,24] and according to the Driver-Pressure-State-Impact-Response(DPSIR) framework to achieve the study’s objectives [21].
Statistical analysis
The IBM SPSS Statistics 27.0 software was used to perform the statistical analysis. Descriptive statistics, including frequencies and percentages of participants’ responses, were calculated. The Independent Samples t-test and a one-way analysis of variance (ANOVA) were applied along with the Chi-Square test to identify factors associated with the public’s knowledge and practices relating to PM2.5 in Bahrain. A p-value of less than 0.05 was considered as statistically significant.
Ethical considerations
This study was approved by the Research and Ethics Committees of the College of Graduate Studies at Arabian Gulf University.
Results
The results of the analysis show that the majority of the participants were Bahraini, with women aged 31–50 years with incomes below BHD 1,500 (USD 3,978) being the predominant group. The majority of the participants held a university degree and worked in the public sector Table 1.
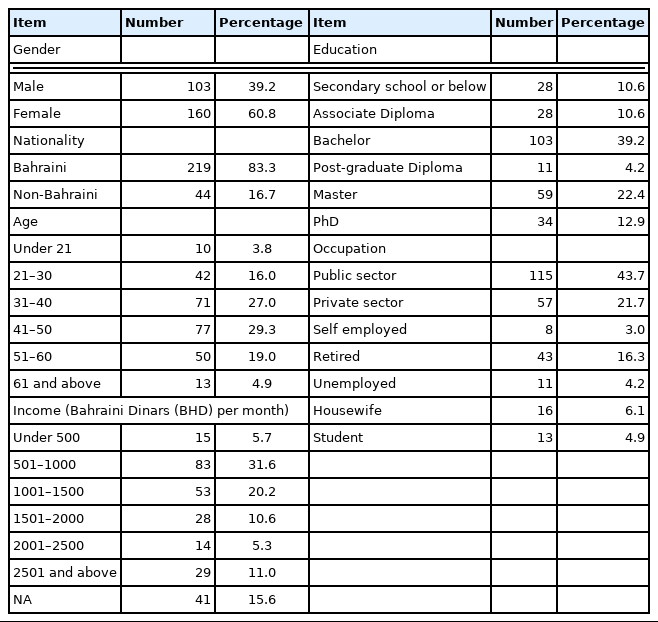
Demographics of participants.
The majority of the respondents (58.2%) stated that they were not aware of the sources and effects of PM2.5, and 43.7% of the respondents did not know whether the PM2.5 concentration in Bahrain was high. Around two-thirds of the respondents reported not knowing whether PM2.5 is measured in Bahrain (Table 2).
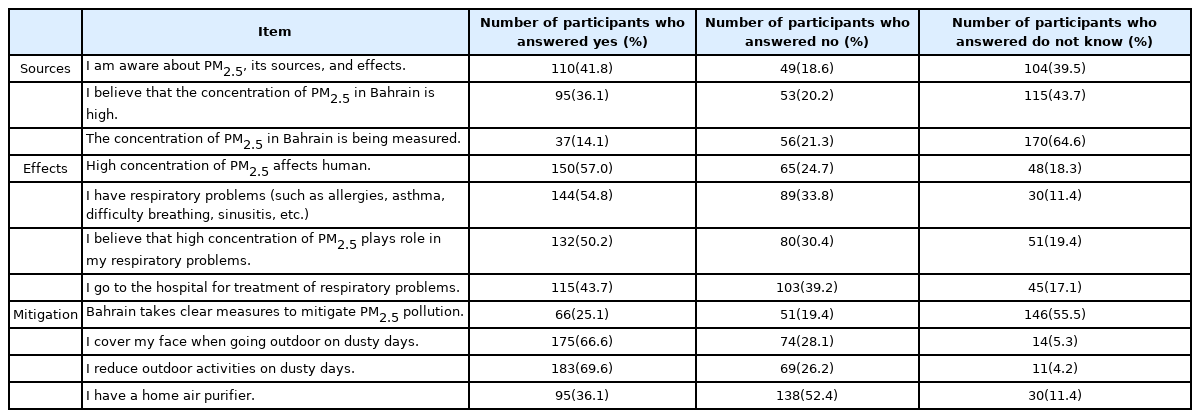
The participants responses to questionnaire items on PM2.5 sources, effects, and protective measures (n=263).
As shown in Table 2, more than half of the respondents (57%) believed that people are affected by exposure to PM2.5. Of the total respondents, 54.8% reported having respiratory problems, and 50.2% believed that a high concentration of PM2.5 played a role in their respiratory problems, with 43.7% requiring hospital treatment for these problems.
More than half of the respondents (55.5%) were unsure whether the government of Bahrain had taken any measures to improve air quality and reduce the concentration of PM2.5. However, two-thirds of them took protective measures, notably covering their faces (66.6%) and reducing outdoor activities (69.6%), with a minority of respondents (36.1%) reporting the use of air purifiers at home Table 2.
The results revealed that there were significant differences among the respondents relating to the precautionary measures they took against poor air quality that were based on several factors. For instance, there were statistically significant differences relating to the use of face coverings and reducing outdoor activities during dusty days according to the participants’ awareness (p<0.05), their beliefs that the PM2.5 concentration in Bahrain is relatively high (p<0.001) and that PM2.5 affects human health (p<0.001), existing respiratory problems (p<0.01), and the belief that PM2.5 is causally linked to their respiratory problems (p<0.001). There were also statistically significant differences relating to the ownership of home air purifiers according to the respondents’ belief that high concentrations of PM2.5 affect human health (p<0.001) and the need for hospital treatment (p<0.001).
Most of the participants consider dust storms (80.6%) and vehicles (65.4%) as the main source of PM2.5, followed by construction and reclamation (54.8%), industries (40.3%), power plants (24.7) and agricultural burning (18.6%). The respondents believed that PM2.5 has respiratory (92.8%) and cardiovascular (31.2%) health effects. Nine participants mentioned other associated health effects relating to neurological and dermatological issues, but none of them mentioned diabetes. Moreover, 75.3% believed that it has environmental effects. The majority of the respondents believed that it is the responsibility of industries (85.6%) and the government (81.7%) to improve air quality, with fewer respondents stating that improved air quality was the responsibility of individuals (60.8%) and non-governmental organizations (NGOs) (49.4%). A minority of respondents (35.4%) viewed improving air quality as a shared responsibility of all concerned parties Table 3. Ten participants held the view that nobody was responsible for improving air quality.
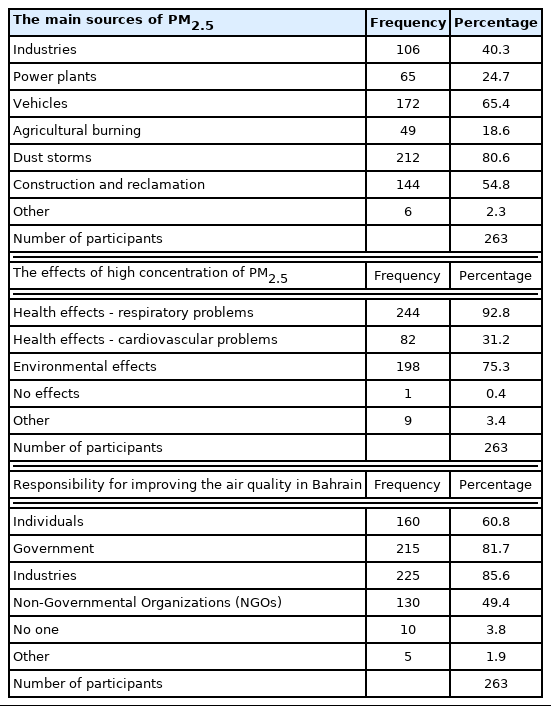
Participants’ perceptions of the sources and effects of PM2.5 and who is responsible for improving air quality.
A significant proportion of the participants in this study (31.9%) expressed willingness to pay to improve air quality in Bahrain. An open-ended question was asked about the amount they would be willing to contribute and the responses were then grouped based on the minimum and maximum of the responses. Among those who were willing to pay, 44 participants (16.7%) indicated their willingness to make monthly payments below BHD 10 (USD 26.5). Of the remaining participants, 15.2% indicated their willingness to make monthly payments ranging between BHD 10 (USD 26.5) and BHD 30 (USD 79.6) (Table 4).
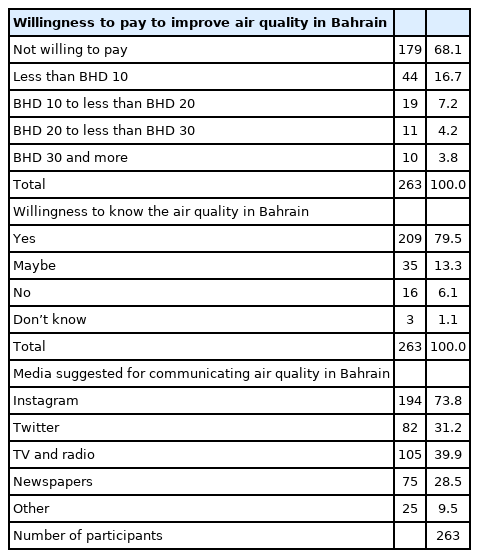
Participants’ interest in knowing about Bahrain’s air quality and their willingness to pay to improve it.
Approximately 79.5% of the participants expressed an interest in knowing Bahrain’s air quality status, with 73.8% stating a preference for Instagram as a social media source of information. Other forms of media were less favored, with a significant percentage of participants indicating a preference for television and radio (39.9%) and newspapers (28.5%) (Table 4).
The respondents recommended a number of measures to improve air quality in Bahrain, including planting trees, measuring the Air Quality Index (AQI) and communicating readings to the public, reducing traffic, and establishing industries away from residential areas. They also suggested raising awareness on how the public can contribute to improving air quality and the precautions that should be taken when the air quality is bad.
Discussion
Air pollution dose not only affect human health but also mental health and welfare. Therefore, the public should be considered as users of air, contributors to improved air quality, and evaluators of the success of air quality policies [15]. From this perspective, health and environmental policies should be aimed at raising the awareness of members of the public and increasing their knowledge about the sources and impacts of PM2.5. The results of this study suggest that such knowledge can contribute positively to the widespread adoption of self-protective measures when the air quality is bad. Whereas the participants in this study who suffered from respiratory problems reported taking such precautions, the participants’ demographic profiles did not influence their adoption of precautionary measures. Another study similarly reported that asthma sufferers frequently checked the air quality, especially when performing outdoor activities, but it did not find any significant associations among public perceptions of air quality and demographic characteristics, namely age, sex, or education level [23].
Considering the public as partners within initiatives to improve air quality would have beneficial effects. The public can effectively contribute to efforts to reduce air pollutant emissions from vehicles and power stations, which are the main sources of PM2.5 in Bahrain, as a result of efforts to raise public awareness about PM2.5 sources. Several participants explicitly stated their willingness to contribute to such efforts following information dissemination on this topic. Studies have identified vehicles as key sources of PM2.5 in the San Joaquin Valley-California [22] and in China [19]. These findings can be disseminated to persuade the public to opt for more sustainable transport options to protect their health.
Another indicator of the participants’ willingness to contribute to improving air quality in Bahrain was their willingness to pay to achieve this outcome. The amounts that they were willing to pay were differentiated according to their monthly incomes, with individuals in the highest income bracket with a monthly income of BHD 2,501 (USD 6,633) and above being more willing to contribute. However, around one-third of the participants who were willing to pay were from lower income groups, with monthly incomes of less than BHD 1,000 (USD 2,652). Nonetheless, the percentage of participants who expressed their willingness to pay for improving air quality was relatively low. Whereas approximately 32% of the survey participants in Bahrain expressed interest in paying for improved air quality, around 78.2% of participants in a Chinese study were willing to pay [19]. Residents who appeared to be more vulnerable to the health effects of air pollution in China were also more willing to pay for air quality improvements [15], whereas no such relationship was identified in Bahrain.
The public should be informed about the links between the quality of the environment and human health. Bahrain’s success story in combating COVID-19 pandemic and raising awareness about the pandemic among different groups within the public domain could provide a role model for dealing with all health-related issues. Bahrain adopted strict measures since the beginning of the pandemic, including closure and prohibition of mass gathering along with increasing the public awareness of the importance of hygiene and social distancing through local and social media. A specific smartphone application was used to communicate between the health authorities and the public [26,27] estimates reported in the literature suggest that in 2019, the relatively high PM2.5 concentration, which is linked to several diseases, could have resulted in 624 deaths in Bahrain [12]. The survey participants in this study suggested several measures and policies to improve air quality in Bahrain resembling those applied while combating COVID-19 pandemic, including working and studying from home. Finding innovative solutions to reduce air pollution has become essential.
The Kingdom of Bahrain has developed an air quality strategy that is in the process of being approved and implemented [28]. However, actions at the strategic level to achieve sustainability should be considered not only in relation to health and the environment but also in the wider context of fossil fuel use, agriculture, industry, and transportation. Air pollutants should be measured, and the Air Quality Index (AQI) should be disseminated along with recommended actions for sensitive groups during days of low air quality, such as studying or working from home. Precautionary measures should be communicated to members of the public who can then adopt practices to reduce the health impacts of air pollution, especially given that a significant number of participants expressed willingness to pay for improved air quality.
To the best of our knowledge, this is the first study to be conducted in a GCC country that investigates public perceptions towards PM2.5. However, it had a number of limitations. The sample size was relatively small, and the number of non-Bahraini participants was limited. These constraints can be overcome in future studies by surveying a larger sample that is statistically representative of all groups (nationals and non-nationals). Moreover, the geographical scope of future studies can be extended to cover all of the GCC countries.
Conclusions
This study is the first to investigate public perceptions relating to PM2.5 in Bahrain. The findings showed that although a considerable number of participants were not informed about PM2.5, the belief that it has negative impacts on human health was widespread. It is important to raise the awareness of the public, especially those who do not currently suffer from respiratory diseases to persuade them to adopt precautionary practices before they develop any of these health problems. Additionally, and from the perspective of shared responsibility, raising public awareness on how to contribute to improve air quality should be prioritized. Although a significant number of participants were willing to contribute financially to improving air quality, the public’s contributions via reduced power consumption and car use need to be communicated to the public. A recommendation of this study is the implementation of a large-scale survey that covers all of the GCC countries and identifies potential areas of collaboration. A second recommendation is to conduct epidemiological studies to advance understanding of the specific cause-effect relationship between air quality and diseases in the GCC countries in general and in Bahrain in particular. Future studies could also explore the economic costs of air pollution impacts, focusing on public health and wellbeing to inform decision makers regarding the importance of the linkages between health and the environment in contexts characterized by reliance on fossil fuel.
Acknowledgement
Authors thank R. Johari for editing a draft of this manuscript.
Notes
This research received no funding and we declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
CRediT author statement
MA: Conceptualization, Methodology, Software, Data curation, Writing-Original draft preparation, Visualization, Investigation, Supervision, Writing-Reviewing and Editing; SA: Data curation, Writing-Original draft preparation, Supervision, Writing-Reviewing and Editing.