Directions for and prospects of the Environmental Health Study in Korean National Industrial Complexes (EHSNIC): A proposal for the third phase of the EHSNIC
Article information
Abstract
The Environmental Health Study in the Korean National Industrial Complexes (EHSNIC) is a project that aims to monitor the exposure and health effects of environmental pollution among residents of national industrial complexes, as well as propose appropriate environmental health measures. Since its launch in 2003, this project has been initiated in eight national industrial complexes. Currently, it is necessary to review the accomplishments and limitations of the phases 1 and 2 of this project, and establish the direction of the upcoming the phase 3. Thus, the present study has developed principles and goals for the phase 3, considering the rationale and justification of the EHSNIC, and presented specific research contents accordingly. In the phase 3, it is important to improve the methods for exposure assessment and evaluation of health effects, in order to identify clearly the association between the pollutants released from industrial complexes and their health impacts, to develop and to reinforce communication strategies to promote participation of residents of communities near industrial complexes. Nonetheless, it is also important to maintain the basic goal of continuously monitoring the level of exposure to and health effects of environmental pollutants.
INTRODUCTION
A large number of studies across the world have assessed the adverse effects of exposure to environmental pollutants produced in industrial complexes among residents of nearby communities [1]. Since the Onsan incidence that occurred in the Onsan National Industrial Complex in Ulsan in 1982, environmental pollution and related accidents in industrial complexes have emerged as important social issues. However, a significant number of studies to date, have merely investigated the level of external environmental exposure of pollutants released from industrial complexes, with only limited studies assessing the level of internal exposure or examining their association with illnesses [2-11].
In this context, the Environmental Health Study in the Korean National Industrial Complexes (EHSNIC) conducted by the Ministry of Environment in Korea since 2003 aims to monitor exposure and health effects of environmental pollutants among residents of national industrial complexes as well as propose appropriate measures for environmental health issues. The phase 1 of the EHSNIC was conducted from 2003 to 2010 in national industrial complexes in Ulsan, Sihwa/Banwol, Pohang, Gwangyang, Yeosu, and Cheongju/Daesan. The year of initiation varied for each complex, with a project launched in 2003 in Ulsan, in 2006 in Sihwa/Banwol, in 2006 in Gwangyang/Yeosu, in 2009 in Pohang, and in 2009 in Cheongju/Daesan. The phase 2 was conducted in the same regions in order to ensure continuity of the phase 1, from 2011 to 2016. As of 2017, the EHSNIC is currently at pilot stage in order to specify the direction and objectives of the phase 3.
Although the accomplishments of the phases 1 and 2 are remarkable, it is difficult to conclude that the demands of various stakeholders such as communities near industrial complexes, corporations, and local governments, have been met. Thus, this study aimed to establish the principles and objectives of the phase 3 of the EHSNIC by evaluating the achievements and limitations of the phases 1 and 2, and to identify specific directions for the phase 3 accordingly.
METHODS
This study conducted a literature review based on annual reports for the phases 1 and 2, and reports evaluating the EHSNIC [12-14], and an expert survey [14]. The purpose of this study is to discuss and propose the direction of the EHSNIC as a core project in the industrial complexes. This study focuses on qualitative assessments as opposed to quantitative assessments, and on research methodology as opposed to quantitative results. The outcomes of the phases 1 and 2 were reviewed, and their accomplishments and limitations were assessed on the basis of the information obtained from the literature review. Additionally, an expert survey was conducted to identify the direction of the upcoming phase 3. Specifically, the principles and objectives of the phase 3 of EHSNIC was established after reviewing the rationale and justification of the EHSNIC, and research contents of the phase 3 were presented accordingly.
The phases 1 and 2 of the EHSNIC were evaluated in terms of legal basis, budget, objectives, external exposure assessment (i.e., concentration of pollutants in environmental media in contact with humans), internal exposure assessment (i.e., measurement of the amount of pollutants introduced into the body in biological specimens such as blood and urine), evaluation of health effects, risk assessment, major accomplishments, and major limitations.
Expert survey was conducted in two rounds, with the second round conducted using only the experts who responded to the first survey. The experts were limited to the fields of environmental and occupational health. The surveys consisted of items rated on a five-point scale (absolutely disagree, disagree, neutral, agree, absolutely agree) as well as open-ended questions.
In the first survey, we collected experts’ opinions on the appropriateness and usefulness of the items for evaluation of the phases 1 and 2, and on the overall direction of the phase 3 of the EHSNIC. In the second survey, we presented more specific measures for the phase 3 of the EHSNIC asking experts to indicate the degree of their agreement with the measures and present additional opinions. The specific direction of the phase 3 consisted of items such as the objective, study design, cooperation with other environmental health studies and projects, risk communication, and management of the phase 3. Twenty-seven experts participated in the first survey, but only 11 of them participated in the second one.
Opinions from local residents, gathered as part of the project to evaluate the phase 2 of the EHSNIC in 2016 [14] were also reviewed with regard to the rationale and justification of the EHSNIC.
RESULTS AND DISCUSSION
Rationale and justification of the EHSNIC
The EHSNIC investigates the entire process from the release of pollutants in industrial complexes to their health effects, and try to find the association between human exposure to pollutants originated from industrial complexes and environmental diseases. In addition, it sheds light on the points that need intervention, through monitoring of the entire process, and further establishes grounds to implement measures to lower the amount of pollutant release, or initiates detailed investigations to verify the association between environmental pollution and health risk. The rationale and justification of the EHSNIC can be examined on a legal basis, as well as in terms of the demands of the residents near industrial complexes and significance for public health.
Legal basis
There is a clear legal basis for the EHSNIC. The primary basis is the regulation of epidemiological study for environment-related health risk stipulated in Article 15 of the Environmental Health Act enacted in 2008 [15]. The year of initiation of the phase 1 was 2003 for Ulsan, 2006 for both Sihwa/Banwol and Gwangyang/Yeosu, which was before the enactment of the Environmental Health Act in 2008. In contrast, the phase 1 projects in Pohang and Cheongju/Daesan as well as the phase 2 projects that began in 2011 were supported by a clear legal basis of Article 15 of the Environmental Health Act. The same legal basis supports the phase 3 of the EHSNIC.
Demands of residents near industrial complexes
According to a survey on resident representatives and a focus group interview conducted as part of the project to evaluate the phase 2 of the EHSNIC in 2016 [14], residents in communities near industrial complexes raised several concerns about the EHSNIC; however, they wanted the EHSNIC to continue. They felt that the EHSNIC should be tailored to the unique features of each industrial complex and expressed their need for more feedback of the results from the EHSNIC. The residents even wanted specific measures, such as regulation of the total amount of pollutant release, preservation of green belt, and emigration of residents, to be developed based on the results from the EHSNIC.
Significance for public health
From a public health perspective, it is very significant to continue monitoring the concentration of environmental pollutants in environmental media, to examine their associations with potential health effects on residents of nearby communities and to implement valid response measures through the EHSNIC. Results from the EHSNIC may serve as the basis for various measures, to address health issues in industrial complexes in the future. In addition, it must be noted that the EHSNIC should be continuously performed as drawing clear conclusions may be difficult in short-term period.
Achievements and limitations of the phases 1 and 2 of the EHSNIC
The assessed achievements and limitations of the phases 1 and 2 are shown in Table 1. Article 15 of the Environmental Health Act serves as a clear legal basis for both the phases 1 and 2. Although the budget used for the phase 2 was slightly lower than that of the phase 1, about 5.3 billion KRW, 6.2 billion KRW respectively, they were more or less similar, considering that the budget calculation for the phase 2 excluded the expense for heavy metal analysis [15]. Whereas the specific objective of the phase 1 was to monitor health effects by establishing a cohort and performing repeated health check-ups for residents in the industrial complexes, that of the phase 2 was to expand the monitoring of environmental pollution and assessment of exposure and health effects. The reasons for the great change in specific objectives were that the phase 1 cohort mainly consisted of teens and female, the check-up method and results were not standardized, and the percentage of participation in repeated follow-ups was low. For example, the participation rate was around 40% in Ulsan and Pohang, 25% in Sihwa/Banwol, and 30-40% in Gwangyang [12].

Summary of the phases 1 and 2 and implication for the phase 3 in Environmental Health Study in the Korean National Industrial Complexes (EHSNIC)
While external exposure was assessed mainly on the basis of air pollution data in the phase 1, chemical substance emission data were additionally used and air pollution dispersion modeling was performed in the phase 2. Further, in the phase 1, internal exposure was assessed mainly by measuring urinary concentrations of heavy metal, cotinine, and 1-hydroxy pyrene (1-OHP) which is one of metabolites of polycyclic aromatic hydrocarbons (PAHs); however, volatile organic compounds (VOCs), PAHs, and phthalates were added in the phase 2, with the same substances measured across all industrial complexes. Regarding the evaluation of health effects, the phase 1 focused on health check-ups and questionnaire survey, while the phase 2 conducted questionnaire survey without health check-ups focusing on linkage to secondary data such as mortality date, cancer registry, and national health insurance data. In addition, risk assessments based on environmental measurement of formaldehyde, arsenic, and ultrafine particles (PM2.5) were also conducted in the phase 2. According to the comprehensive evaluation of the phase 2 [14], substances such as lead, nitrogen oxide (NOx), trichloroethylene, styrene, nickel, manganese, chrome, benzene, xylene, cadmium, and arsenic were identified as substances requiring continuous monitoring or new investigation, though they vary across industrial complexes. Furthermore, although they also vary across industrial complexes, diseases such as hypertension, diabetes mellitus, chronic lower respiratory diseases, cancer, anemia, allergic dermatitis, and asthma were identified in higher frequencies in exposed areas, thus requiring an investigation on causality.
The major achievements of the phase 1 were establishing a cohort of residents near industrial complexes, initiating communication with the local communities regarding health concerns affecting residents in industrial complexes, and establishing and strengthening a foundation for investigating and researching vulnerable areas in Korea. The major achievements of the phase 2 were applying a standardized protocol to overcome the limitation of using different methodologies for various industrial complexes in the phase 1, actively performing environmental and biological monitoring as well as modeling to assess exposure and evaluating health effects by linkage to multiple types of secondary data.
On the other hand, the major limitations of the phase 1 include the issue of representativeness for the established cohort, low proportion of follow-up health check-up, lack of standardized protocol, inadequate environmental monitoring, limited use of disease data, and inadequate feedback for policy utilization. The phase 2 was limited in terms of individual exposure assessment, inadequate database management, study design to assess association between exposure and disease, and risk communication. Despite these limitations, however, the phase 1 of the EHSNIC is meaningful considering that it established a foundation for the EHSNIC and increased awareness of improving the environment among local residents. The phase 2, though limited, obtained results that suggest significant release of industrial pollutants and their association with health effects among residents.
Expert survey results
In the first expert survey, experts stated that the phases 1 and 2 of the EHSNIC made significant contributions in increasing the awareness of the importance of environmental improvement but were inadequate in terms of identifying a causal relationship between environmental exposure and health of residents in the industrial complexes. In addition, experts suggested that the phase 3 should focus on environmental pollution monitoring, cohort development and management, biological monitoring, risk communication, and use of new methodology for exposure assessment. Many experts believed that the phase 3 should establish a clear and customized objective for each industrial complex, develop a systematic database and enable open access to it, and utilize study results to increase and improve awareness among stakeholders. On the contrary, only a few experts mentioned that methodologies for exposure assessment and evaluation of health effect should be improved or that more national industrial complexes should be included in the study.
Experts’ suggestions on the direction of the phase 3, as established in the second expert survey, are shown in Table 2. Experts generally agreed to the overall items, including the objective, study design, cooperation with other environmental health surveys, risk communication, and management. In particular, 100% of the responded experts agreed that the objective of the phase 3 should be set on ‘identifying environmental health problems (identifying association between exposure and health effects)’ and ‘developing environmental health measures. Also, they agreed that opinions from stakeholders (communities near industrial complex, corporations, and local governments) should be collected when developing environmental health measures. However, certain experts remained neutral to or disagreed with certain items, such as establishing a retrospective cohort or selecting comparison groups.
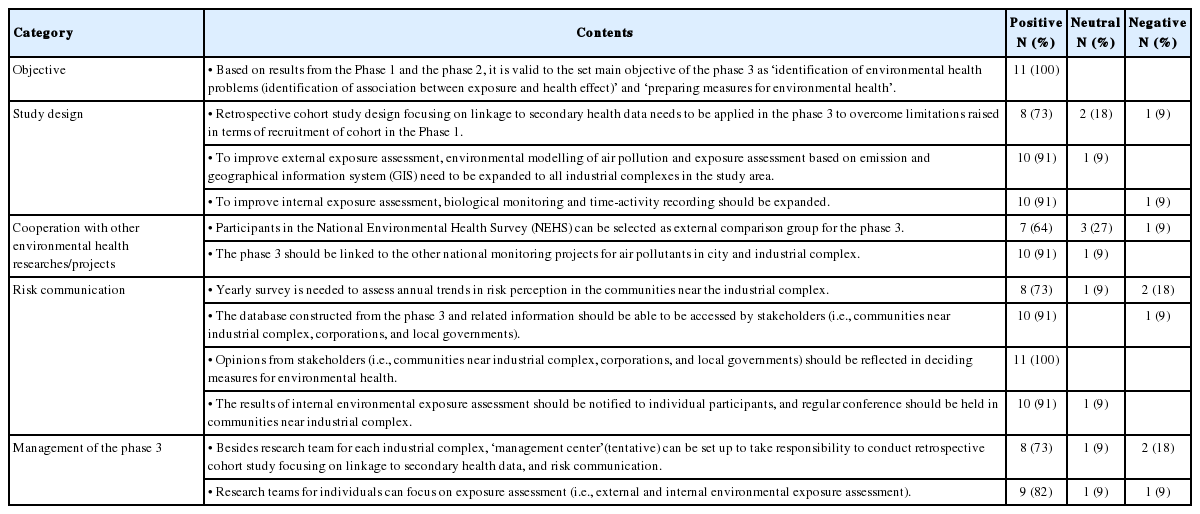
Opinion and perspective for the phase 3 of the Environmental Health Study in the Korean National Industrial Complexes (EHSNIC). (Results from the 2nd expert survey)
Suggested direction of the phase 3
The direction of the phase 3 of the EHSNIC is suggested as follows, based on the rationale and justification of the EHSNIC, evaluation of the phases 1 and 2, and expert opinions.
Principles of the phase 3 of the EHSNIC
Based on the assessment of the phases 1 and 2 and survey of residents near industrial complexes and experts, we suggest the phase 3 of the environmental health study to be defined as a resident-participation project, namely “EHSNIC in industrial complexes in cooperation with residents of the areas.” In order to strengthen participation of residents, risk communication and voluntary participation by residents must be ensured throughout the project. To this end, the concepts and cases of “resident-participation” or “region-specific” health promotion activities, launched in recent years, can be benchmarked [16-17]. Furthermore, it is desirable to reflect on other principles adopted by the Environmental Health Act, such as recipient-focused (oriented), susceptible population-prioritized, and precautionary principle [18].
Objectives of the phase 3 of the EHSNIC
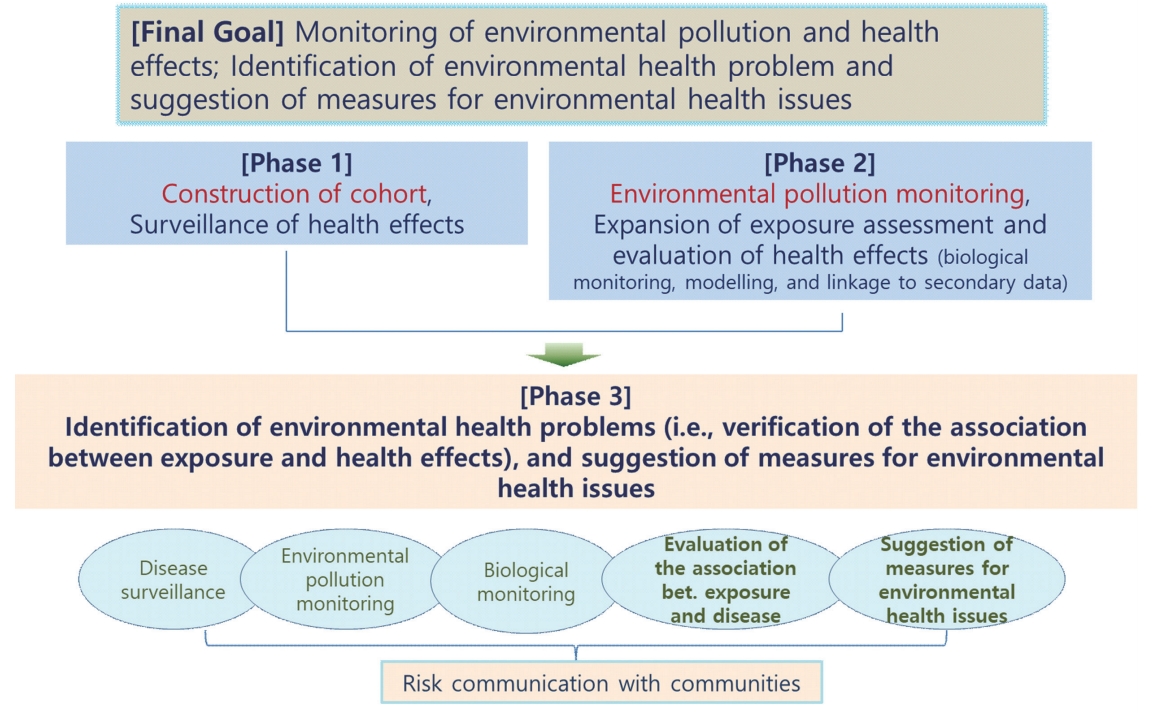
The overall objective of the environmental health study is to monitor environmental and its health effects, and to identify environmental health problems in order to present appropriate environmental health measures. It seems valid to include the specific goals of the phases 1 and 2 as well as the overall objective of the EHSNIC, while we focus on evaluating the association between exposure and disease, and develop environmental health measures (Figure 1). The phase 1 focused on establishing a cohort, while the phase 2 focused on monitoring environmental pollution. Hence, the phase 3 should be focused on identifying environmental health problems and developing environmental health measures in order to achieve the overall goal. By doing so, it would be possible to advance the achievements of the phases 1 and 2 to the phase 3 and integrate all the progresses.
Suggested objectives for the phase 3 of the EHSNIC
In fact, a proposal including ‘drawing of conclusions on environmental health concerns’ was presented as part of a masterplan proposal for the phase 2 (proposals 1-5) in 2011 [12]; however, this is actually the final goal of the EHSNIC and is difficult to achieve. Therefore, it seems valid to set this as the objective of the phase 3, with the assumption that it could be achieved based on the accumulated data and methodological experiences of the phases 1 and 2.
In addition, the specific objectives of the phase 3 could be set to ‘diseases surveillance,’ ‘environmental pollution monitoring,’ ‘biological monitoring,’ ‘evaluation of the association between exposure and disease,’ and ‘suggestion of measures for environmental health issues’. And these objectives should be achieved promoting ‘risk communication with communities,’ that is in reflection of the demands of the residents near industrial complexes.
Contents of the phase 3 of the EHSNIC
Selection of regions
Fundamentally, the phase 3 should maintain the same regions as in the phases 1 and 2 (i.e., Ulsan, Sihwa/Banwol, Pohang, Gwangyang, Yeosu, and Cheongju/Daesan). Because it is difficult to say that definitive conclusions have been drawn from the EHSNIC, focusing on the previously investigated regions seems more desirable than expanding to other regions. However, it may be necessary to select additional regions from the aspects of previous selection criteria such as social issues, size of industrial complex, type of industry, and regional distribution. Furthermore, it would be important to include additional industrial complex regions in which leakage accidents occurs or complaints are brought, or to prepare to launch an expanded or separate project in the future.
Selection of substances for monitoring
In the phase 2, the major pollutants identified were heavy metals, VOCs, PAHs, carbonyl compounds, and PM, though the types of industries in each complex varied. In the phase 3, continuous monitoring should be maintained within the scope of the budget, and the changes of pollutants (amount of emission) among regions should be reviewed and reflected. In addition, selecting substances perceived by residents to be hazardous may be an option as well.
Selection of control (comparison) group
Use of air pollution modeling
In the phase 1, the regions of exposure or control were defined based on a particular distance from the corresponding industrial complex; however, this criterion varied across complexes and even within the same region [12]. In the phase 2, separation of exposure and control regions was attempted via air pollution modeling using information such as wind direction. However, such an air pollution modeling technique was not applied in certain regions, and it was not established as a standard method [14].
In the ‘Pilot study for air pollution prediction modeling for environmental epidemiological study’ in the final report of the project to evaluate the phase 2 of the EHSNIC in 2016 [14], seasonal average level of air pollutants was mapped using the Community Multi-scale Air Quality model (CMAQ) over the Ulsan industrial complex. It was to assess the contribution and area of influence of air pollutants emitted from the industrial complex. Residents’ exposure to these pollutants was also assessed using the results of this modeling. By this approach, it was possible to obtain evidence supporting scientific selection of exposure/control regions and confirm that this data can be used to assess individual exposure for environmental epidemiological studies. In the phase 3, this modeling technique may be applied to all the study regions to select the control (comparison) groups.
Use of National Environmental Health Survey data
If the biological markers measured in the phase 3 are substances that are measured in the National Environmental Health Survey (NEHS), it is possible to set the results of the NEHS as the comparison group, regarding them as a level of representative exposure of Korean. In fact, heavy metals, VOCs, and PAHs are measured in both the NEHS and in the EHSNIC [19]. Cooperation with other national projects has benefits in terms of utilizing the established infrastructure of environmental health-related surveys.
Development of standardized protocol
In the phase 2, a standardized study protocol was developed and applied based on the experiences from the phase 1; however, a more detailed standardization process is required for the phase 3. For instance, although the same questionnaire items were used in the phase 2, the order of the items varied among the different industrial complexes. In addition, questionnaire items added to each industrial complex also varied. A standardized protocol is needed for questionnaire items and also for coding guidelines, collection, storage, and analysis of environmental and biological specimens, exposure modeling, and evaluation of health effects using secondary data that could be applied across all industrial complexes. A standardized method should also be applied in establishing, refining, and using a comprehensive database. Furthermore, a standardized protocol should be developed for risk communication, which is one of the items emphasized in the phase 3, in terms of contacting residents, holding conferences with stakeholders, and sharing data.
The ‘EHSNIC Management Center” (tentative) could take charge of developing standardized protocols. And instruments as well as procedures used in the existing NEHS could be utilized. The third NEHS also underwent a standardization process, where the questionnaire items were matched with those used in the National Health and Nutritional Examination Survey (NHNES) [19].
Improvement of methods for exposure assessment and evaluation of health effects
Exposure assessment
In the phase 3, the major substances to be measured need to be selected for each industrial complex, and air pollution modeling based on air monitoring or emission data need to be expanded. To this end, we concluded that the CMAQ model, applied to the Ulsan industrial complex in the project to evaluate the phase 2 of the EHSNIC [14], could be expanded to all the industrial complexes.
Substances to be placed under biological monitoring in the phase 3 could be identified in connection with external environmental exposure assessment. When selecting control regions for each substance, the results of modeling or the NEHS could be used. Time-activity recording could be used for individual exposure assessment, particularly on subjects under biological monitoring. Further, a study design that enables examination of longitudinal changes through repeated followups could be applied to subgroup of participants.
The phases 1 and 2 mainly used an approach in which exposure and control regions were simply selected and compared; however, the phase 3 should comprehensively utilize data and resources such as distance, geographical information system (GIS), air pollution modeling, and time-activity recording to assess the level of exposure at individual level. In other words, a study design more effective for identifying associations, as opposed to ecological methodologies, is needed, and this could be achieved by enabling assessment of dose-response relationship using individual exposure data.
Evaluation of health effects
A longitudinal observational study is essential to clearly identify health effects and to overcome unclearness of regional comparison and in terms of temporality in the association observed between exposure and disease in the phases 1 and 2 [20].
Considering practical conditions, such as research funds, it could be a useful approach to focus on exposure assessments using addresses. Addresses were included in the existing database to evaluate association with health effects based on secondary data generated since the phase 2 [21]. This approach could be referred to as a ‘big-data based follow-up study’, which is fundamentally an expansion of the method for evaluation of health effects with linkage to secondary data in the phase 2. One significant difference is that the phase 2 was limited to regional comparisons, whereas the big-data based follow-up in the phase 3 is designed to assess the association between individual levels of exposure and health effects.
Subjects should be the participants in the phases 1 and 2 who additionally provide consent form for utilization of data containing address histories and other secondary data. The number of consent forms obtained, and the extent of the accessible secondary data, are the key in this matter. Governmental cooperation such as cooperation by the Ministry of Environment may be needed to address relevant legal issues [22]. The newly recruited study participants will be followedup from the past with reference to the beginning of the phase 3, and exposure-disease association will be evaluated between past levels of exposure computed by address-based modeling and level of morbidity or mortality (e.g., national health insurance, mortality data, and cancer registry data). The issues to be considered include the participants of the phases 1 and 2 who moved to another region, the possibility of a subject that they may not have actually lived near an industrial complex, despite their addresses in the area. And characteristics of resident populations by year should be investigated to collect potential confounders.
In addition to big-data based follow-up study, a cross-sectional study or a case-control study design could be integrated depending on the disease interested and conditions of the industrial complex under study. Furthermore, association study could be conducted using effect biomarkers of preclinical stages.
Measures to cooperate with other national surveys
As a way to cooperate with the NEHS, several measures could be considered such as matching questions in questionnaires, sharing of procedures for analyzing biological specimens, and process of public release of data. As a more active measure for cooperation, it could be considered to allocate a larger sample in industrial complex regions for the NEHS. Currently, the NEHS allocates a partial sample (10% of total adults) to regions near the national monitoring site for heavy metals in ambient air. The sites for heavy metal monitoring are generally consistent with regions near industrial complexes [23].
In the long run, cooperation with the NHNES and National Community Survey, and measures to cooperate with the Harmful Pollutant Monitoring in Urban and Industrial Regions, should also be considered.
Risk communication
Local residents’ perceptions of industrial complexes and awareness of the risks of environmental hazardous substances need to be surveyed annually to track changes by year, and the database and relevant data should be shared with stakeholders (e.g., communities near industrial complexes, corporations, and local governments). The results of internal environmental exposure assessment should be notified individually, and conferences with stakeholders should be held periodically. As a more active measure, providing education to improve environment (e.g., guideline to lower exposure) could also be an option. Ultimately, stakeholders’ opinions must be considered before suggesting measures for environmental health issues. Diseases specific to each industrial complex, identified in the phase 2, will be evaluated for exposure-disease relationship in the phase 3 that addresses the limitations of phases 1 and 2. Then the diseases will be ultimately identified as environmental health concerns. This entire process should be accompanied by appropriate risk communication.
Contents related to risk communication should be provided by the researchers of each industrial complex; however, this requires the support and cooperation of the EHSNIC Management Center. Further, it is possible for stakeholders, including local government officials in charge of environmental matters, to participate in the EHSNIC Management Center.
Management of the phase 3
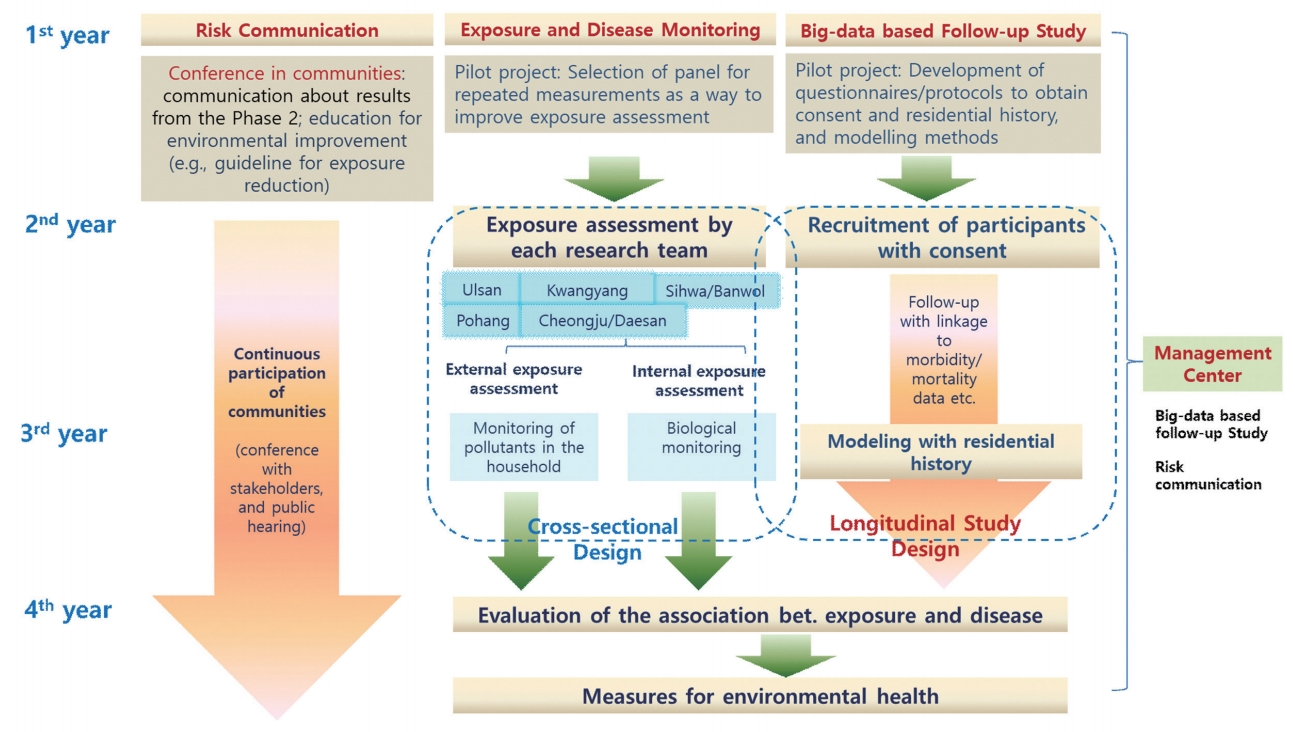
While risk communication, monitoring of exposure, surveillance of disease, and big-data based follow-up are performed for each industrial complex, the EHSNIC Management Center should provide support to facilitate projects in each industrial complexes (Figure 2). The EHSNIC Management Center could cooperate with researchers of each industrial complex by supporting the development of a standardized protocol, big-data based follow-up, and risk communication strategies.
Suggestions for yearly progress and contents of the phase 3 of the EHSNIC
Researchers of each industrial complex should take charge of participant recruitment while the EHSNIC Management Center performs evaluation of health effect based on individual address-based modeling and linkage to secondary data, with active cooperation between the two bodies. Meanwhile, each industrial complex should be led in investigating industrial complex-specific health effects.
If the duration of the phase 3 is four years, the focus in the first year should be on developing strategies for risk communication, exposure monitoring, disease surveillance and conducting a pilot study for big-data based follow-up. For the second and third year, the focus should be performing exposure assessments and recruiting participants as well as obtaining consents in each industrial complex. For the fourth year, the focus should be evaluating the association between exposure and disease and suggestion of measures for environmental health issues (Figure 2). Cross-sectional designs could be used for exposure assessments, which complement the follow-up study design of big-data based follow-up study. Further, various projects should be planned for risk communication in order to promote continuous resident participation throughout the whole period of the EHSNIC.
CONCLUSION
In this study, the achievements and limitations of the EHSNIC were reviewed, and the directions of the phase 3 was proposed, based on the evaluation of the phases 1 and 2. The phase 3 requires improvement in multiple aspects in order to identify environmental health problems and develop environmental health measures while maintaining the basic goals of continuously monitoring of environmental exposure and surveillance of health effects in industrial complexes. To ensure the resident-participating project, risk communication and resident participation must be facilitated throughout all periods of the EHSNIC, and the methods for exposure assessment and health effects should be improved to clearly identify the association between exposure and evaluation of health effects.
Acknowledgements
This study is the modified version of the part, ‘The direction of the phase 3 of the EHSNIC in the final report of the project to evaluate the phase 2 of the EHSNIC in 2016 [14].