




Introduction
The number of patients with allergic diseases in Japan has demonstrated an increasing trend in recent years [1]. The estimated number of patients with asthma increased from 1.10 million in 1999 to 1.12 million in 2017, the number of patients with atopic dermatitis increased from 0.40 million to 0.51 million, and the number of patients with allergic rhinitis increased from 0.47 million to 0.66 million. The social burden of allergic diseases is not only limited to the medical expenditures of the diseases but also includes the decrease in a patient’s quality of life and labor productivity [2, 3]. Therefore, it is important to assess the cause of these increases in allergic diseases and to find methods to prevent them. The representative allergic diseases (i.e., asthma, allergic rhinitis, and atopic dermatitis) are associated with each other, and the comorbidity of these diseases in a patient is relatively common [4]. After developing atopic dermatitis, an infant often develops asthma and allergic rhinitis. This phenomenon is known as atopic march [5]. Environmental factors, such as air pollutants, are believed to be the major cause for allergic diseases [6]. Yokkaichi asthma, which was caused by pollution from petrochemical complexes, emerged in Japan in the 1960s [7], and the massive increase in asthma patients became a social problem. Even in recent years, the association of allergic diseases and particulate matter 2.5 (PM 2.5) or Asian desert dust has gained significant attention in Japan [8]. Exposure to these environmental factors changes depending on the period or birth cohort, and the trend of disease prevalence is considered different not only in terms of periods but also in terms of birth cohorts.
Age–period–cohort (APC) analysis is often used as an analysis method for investigating the trend of disease prevalence [9]. By using APC analysis, we can identify the age, period, and cohort effects on the prevalence of a disease and assess the change of each effect over specified time points. Regarding APC analysis for allergic diseases, APC analysis for asthma has been conducted in some countries [10]. Although APC analysis for childhood asthma had been conducted in Japan [11], the analyzed period was from 1984 to 2004. Therefore, the exact trend of childhood asthma in recent years is uncertain. The cohorts analyzed in this previous study were also relatively limited because the age period of childhood is short. Although the age of onset for the diseases is high in childhood, we can assess not only the trend of prevalence for older age groups but also the trend of broader birth cohorts by analyzing the data of broader age categories. Data from the Patient Survey in Japan are useful because it is a nationwide survey that investigated the number of patients for specific diseases and can be used to assess the trend of allergic diseases. In the current study, we investigated the trend in the prevalence of asthma, allergic rhinitis, and atopic dermatitis in Japan.
Methods
The data of the Patient Survey in Japan [1] was used for APC analysis. The survey was conducted for grasping the number of patients, and it tallied the number of patients who visit a hospital or a clinic at Japan every three years. The hospitals and clinics surveyed were randomly chosen, whereas all hospitals with more than 500 beds were completely surveyed [12]. We used the data of the estimated total number of patients from the seven Patient Surveys conducted from 1999 to 2017. The estimated total number of patients was calculated in the Survey as follows: [12]
(Total number of patients) = (number of hopitalized patients) + (number of first visit outpatients) + (number of returning outpatients) × (mean consultation interval) × (adjustment factor) (1)
Diseases were classified based on ICD-10 codes in the Survey, and the ICD-10 for the allergic diseases are as follows: J45–J46 for asthma; L20 for atopic dermatitis; and J30 for allergic rhinitis.
We calculated the prevalence of each allergic disease per 1,000 people for men and women from 1999 to 2017. The prevalence was obtained by dividing the number of patients by total population in Japan by age groups and years. The data of total population was extracted from the data of the Vital Statistics in Japan [13]. The age groups were defined from 0–4 years to 65–69 years by 5-year increments in the data. Also, we used a Bayesian APC model assuming that an outcome follows Poisson distribution for the analysis [9]. The estimated number of a disease was used as outcome value, and corresponding total population was used as offset term. A first-order correlated random-walk was used as the Bayesian prior distributions for each effect. Additionally, in the APC analysis, those who were 65–69 years old in 1999 (i.e., those who were born in 1930–1934) were the first cohort, as this was the oldest birth cohort in the data set. Through a 1-year shift of the birth years, starting from the first cohort, the age group of 0–4 years in 2017 (i.e., those who were born in 2013–2017) was the last cohort. We used the Hamiltonian Monte Carlo method to estimate the parameters [14]. All statistical analyses were conducted using R version 3.5.1 software [15].
Results
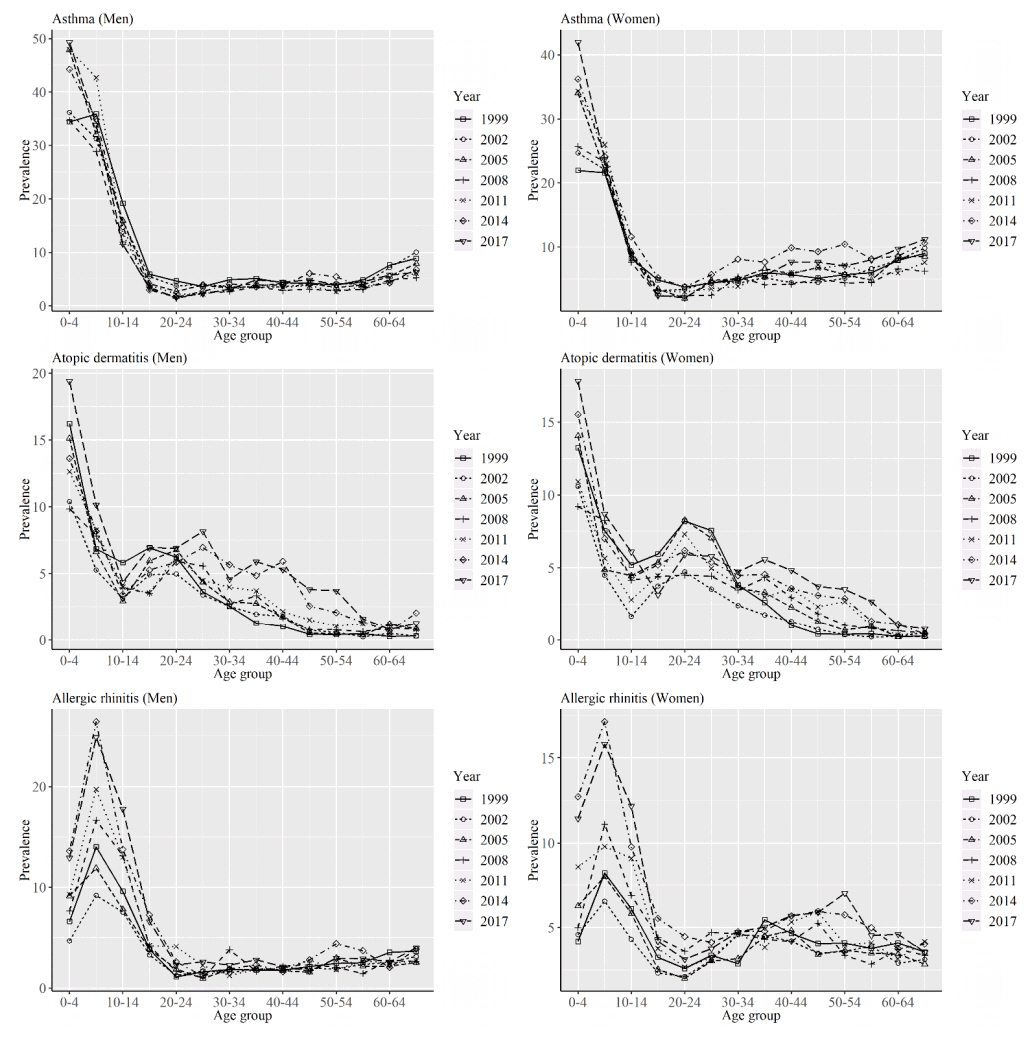
Figure 1 shows the prevalence of each allergic disease per 1000 people for men and women from 1999 to 2017. Although the prevalence of asthma among men increased in the zero- to four-year-old age group from 1999 to 2017, the prevalence decreased in many other age groups. For women, the prevalence of asthma increased in most age groups, particularly in the zero- to four-year-old age group from 1999 to 2017. Regarding atopic dermatitis, the prevalence among men increased in most age groups from 1999 to 2017. For women, the prevalence increased in all age groups, except for the 15- to 29-year-old age groups over the years. The prevalence for allergic rhinitis increased in most age groups over the years for both men and women.
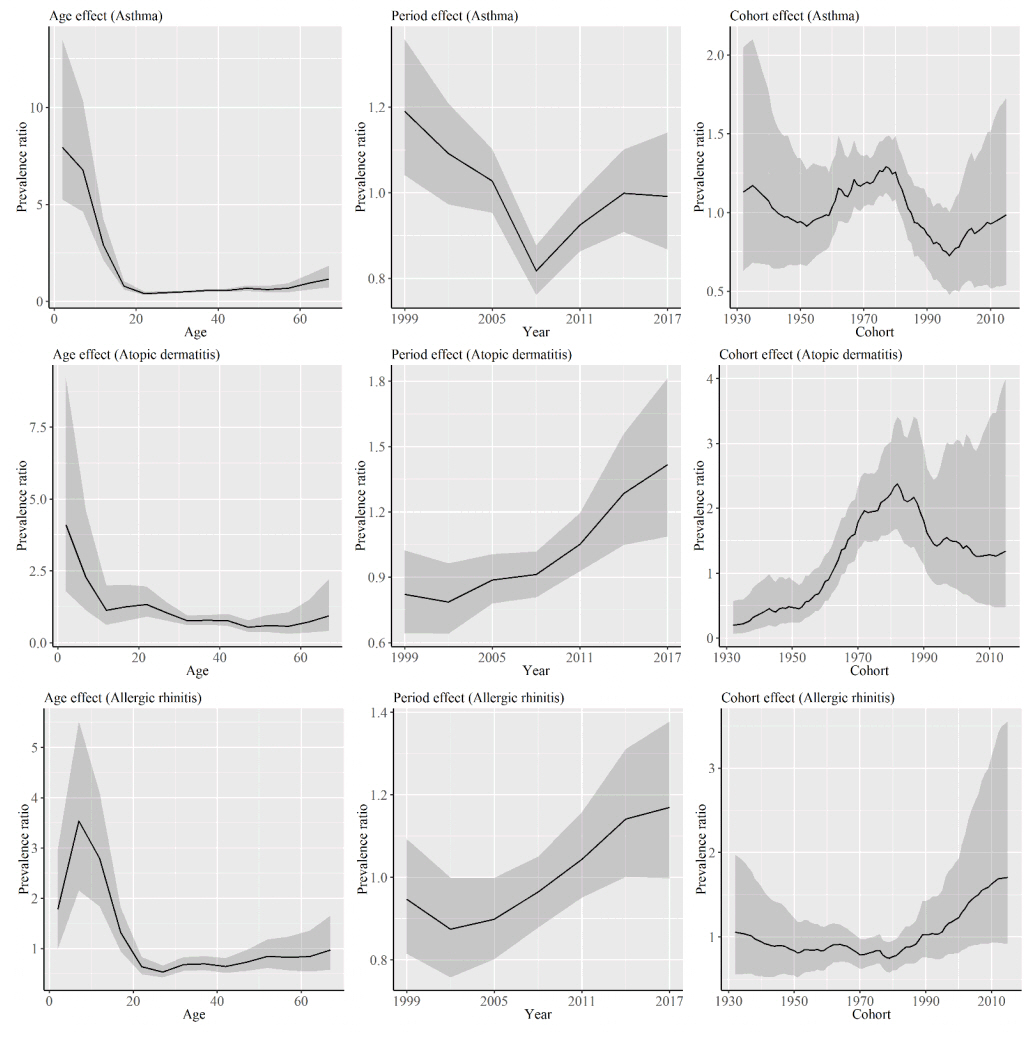
Figure 2 shows the results of the APC analysis for asthma, atopic dermatitis, and allergic rhinitis for men. The age effect for asthma rapidly decreased until 20 to 24 years and then increased steadily thereafter. The period effect for asthma decreased until 2008 and moved toward an increasing trend thereafter. The cohort effect increased from cohorts born in the early 1950s to the late 1970s and then decreased thereafter. The age effect for atopic dermatitis decreased with an increase in age. The period effect for atopic dermatitis consistently increased from 2002. The cohort effect increased, particularly for cohorts born in the early 1950s to the early 1980s, and then decreased thereafter. The turning point of decrease was the same as that for asthma. The peak of the age effect for allergic rhinitis was five to nine years old. The period effect increased beginning in 2002, and the cohort effect began to increase in cohorts born in approximately 1990.
Figure 3 shows the results of the APC analysis for asthma, atopic dermatitis, and allergic rhinitis for women. Although the degree of decrease in the period effect for asthma was smaller for women than for men until 2008, the degree of increase in the effect beginning in 2008 was larger for women. Although there were subtle differences between sexes, the trends of each effect for atopic dermatitis and allergic rhinitis were relatively similar among men and women.
Discussion
Regarding asthma, the age effect showed a slight increasing trend with an increase in age from 20–24 years old, and the prevalence increased in older ages. It is known that the age of onset for asthma is also high in older ages [16], and our results seem to show that prevalence increases in older people. Regarding the period effect for asthma, we observed a difference in the effects among the sexes in terms of the degree of decrease until 2008.
One possible reason for this trend is the rapid decrease of smoking prevalence in men. Smoking prevalence in Japan is higher for men than for women, and smoking prevalence in men has been decreasing in recent years [17]. Smoking is a risk factor for asthma [18], and a decrease in the smoking rate might have contributed to the decrease of the effect. On the other hand, the degree of increase of the period effect from 2008 was larger for women, and the increase was observed in the middle or older age groups (Figure 1). The risk factors for asthma that are associated with adults include stress and alcohol drinking [19, 20]. Diseases that are associated with stress, such as depression or anxiety disorders, have increased over the years [1], and the degree of increase was larger for women. Furthermore, from 2003 to 2017, the prevalence of alcohol drinking decreased for men while increased for women[21]. Therefore, an increase in psychological stress and the prevalence of alcohol drinking in adults might have led to the increase in the prevalence of asthma, particularly for women. Regarding the cohort effect, the effect showed increasing and decreasing trends. Although there are patients who develop asthma as adults, the age of onset is particularly high in childhood, as shown by our results. Therefore, the cohort effect is considered to reflect the exposure to the risk factors of asthma, particularly in childhood. One possible factor that influences the cohort effect is air pollutants. The cohort effect began to increase from cohorts born in approximately 1950 for both men and women (Figures 2 and 3). At that time, Japan experienced rapid economic growth after World War II. A large-scale outbreak of asthma caused by a petrochemical complex (i.e., Yokkaichi asthma) occurred in the 1960s [7], and air pollution became a social problem in Japan in 1970. China also experienced similar levels of air pollution and an increase in asthma patients during a period of economic growth [22]. The economic growth of Japan is considered related to the increase of the cohort effect. The regulation of exhaust gas from motor vehicles [23] or the revision of environmental standards for nitrogen dioxide [24] began in 1978. These regulations for air pollution are considered to have affected the decrease of the cohort effect for cohorts born in approximately 1980.
The period effect for atopic dermatitis demonstrated an increasing trend from 2002. One possible cause is an increase in the population of urban areas in Japan. There are some reports that have shown the associations between urbanization and the increase in atopic dermatitis [25]; this led to the belief that air pollution in urban areas might affect disease development. The cohort effect increased from cohorts born in approximately 1950 to 1980, similar to that of asthma. This is considered related to the emissions of air pollutants accompanied by economic growth.
The period effect for allergic rhinitis also increased beginning in 2002. The development of allergic rhinitis is also high in urban areas [26], and urbanization is one possible cause of this increase. Hay fever is the most common type of allergic rhinitis in Japan, and it has been reported that the scattering amount of pollen has increased in Tokyo over the years [27]. The cohort effect increased from cohorts born in approximately 1980 for men and in the 1980s for women. In the 1950s and 1960s, many Japanese cedar and cypress trees were planted on Japanese islands [28]. This is believed to be the main cause of the increase in allergic rhinitis in Japan, particularly hay fever. The mass scattering of pollen occurs from Japanese cedar trees that are 30 years old and older [29], and this is thought to be related to the trend of the cohort effect. The number of patients with hay fever rapidly increased from the late 1970s to 1980 [30].
Although we used nationwide government statistics data, one limitation of this study is that estimates of the number of patients was used for the analysis. To accurately assess the prevalence of these diseases, an epidemiological study that targets a broader range of age groups should be conducted.
Conclusions
We found that the prevalence of asthma, atopic dermatitis, and allergic rhinitis were different depending on the cohorts. The cohort effects for asthma and atopic dermatitis increased rapidly for cohorts born in approximately 1950 to 1980, and the cohort effects for allergic rhinitis consistently increased beginning around the 1980s. An increase in air pollutants accompanied by rapid economic growth and afforestation in the late 20th century appears to be related to the trends of the cohort effects of the analyzed allergic diseases.