




Introduction
The use of mobile phones has rapidly increased during the last 10 years in Korea. At the end of 2011, the number of mobile phone subscribers exceeded the estimated number of Korean population with approximately 53 million subscribers [1]. Mobile phone technology has pervaded into various corners of our society, giving birth to new lifestyle patterns, and eliciting new social problems, thus, evolving into something much more than a communication tool. This seems to be especially true for adolescents as mobile phones now have a significant impact on their daily lives [2]. Mobile phones are used by adolescents not only to keep in touch with their relatives or friends, but are also used as a platform for expressing one's identity and as a source of entertainment. Mobile phones have become so popular among children and adolescents that problems of mobile phone addiction have newly arisen such that they call for attention from the society [3]. Furthermore, public concerns over possible health problems from intensive use of mobile phones have heightened recently as radiofrequency electromagnetic field radiating from mobile phones has been newly classified as one of group-2B agents in International Agency for Research on Cancer (IARC)'s carcinogen classification [4].
However, despite the fact that Korea is one of the leading countries in the field of mobile phone technology, and with most of the population using mobile phones, only a few studies with statistics are available on this particular issue. The objective of this study was to examine the patterns of mobile phone ownership and use, and related characteristics focused on the socioeconomic position in children and adolescents of Korea. Three data sets collected between 2008 and 2011, ranging from one city data to nationwide data, were used in this study.
Materials and Methods
Datasets and Study Subjects
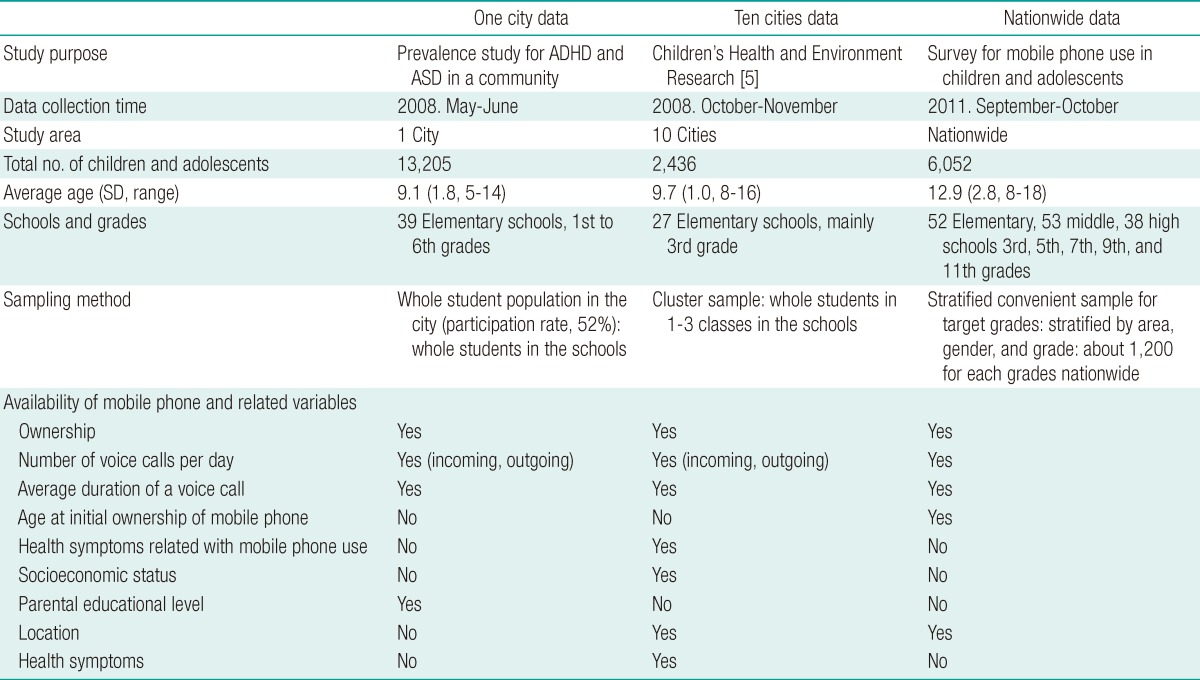
We used three epidemiological datasets which were collected between the period 2008 and 2011 in Korea. Descriptions for each dataset are provided in Table 1. The original purposes to collect those datasets were to examine the prevalence of attention deficit hyperactivity disorder and autism spectrum disorder in a community in the one city data, to examine children's health related with environmental exposure in the ten cities data, and to survey for mobile phone use in children and adolescents in the nationwide data.
The prevalence study is a cross-sectional survey of elementary schools (participation rate: 52% among whole students in the city) in one city during the period 2007-2008 by the Environmental Health Center for Neurodevelopment, Dankook Medical Center, which is one of the 13 Environment Health Centers supported by the Ministry of Environment of Korea. The survey region is a medium sized city with mix of urban, industrial and rural areas. Parents or guardians of participating children responded to a questionnaire delivered by their child/children via school teachers. We used the 2008 data which contained information on mobile phone use in children (13,205 children).
The ten cities data, originally called the Children's Health and Environment Research (CHEER), was a repeated follow-up study of children recruited from 10 cities with stratified convenient cluster sampling for 2005-2010 [5]. A questionnaire was administered to the parents or guardians of participating children. Health examination including blood and urine sampling was undertaken in participating children. The CHEER has information on mobile phone use during the period between 2008 and 2010, when the majority of participating children were 3rd and 5th graders in elementary schools, respectively. We used the CHEER data for 2008 (2,436 children).
After the IARC announced that radiofrequency radiation from mobile phone use is classified into group 2-B, a possible carcinogen to human, a group of researchers supported by the National Assembly and a civic group performed a brief survey on the mobile phone use status of Korean children and adolescents nationwide in 2011 (6,052 children and adolescents).
The three studies of which the data were used in the present study were approved by the institutional review boards of the Dankook University Hospital. Written informed consent was obtained from all participants and participants' parents or guardians after fully informing of the details of the study before enrollment.
Mobile Phone Use Variables
As variables of mobile phone use, information on ownership, number of voice calls per day, and average duration per voice call were available in all three datasets, while age of first mobile phone ownership was available only in the nationwide data. Monthly fee for mobile phone use was used from one and ten cities data.
Variables Potentially Related with Mobile Phone Use
Demographic factors (age or school grade, gender), residential area, parental educational levels and socioeconomic position (SEP) were considered to be potentially related with mobile phone use in children and adolescents. These variables of SEP were not available in the nationwide survey data on mobile phone use. We considered both individual and community levels of SEP. We used monthly household income as an individual SEP through the questionnaire information and the gross regional domestic product (GRDP) per capita in the residential area as a community SEP through GRDP divided by the number of population in the residence registry in 2008 [1]. The variables of SEP were available from the ten cities data and parental educational level from the one city data.
Health Symptoms Related with Mobile Phone Use
Information about health symptoms related with mobile phone use was available in the ten cities data, which included the following 11 symptoms: discomfort, dizziness, dry skin, eye pain, fatigue, headache, impaired concentration, impaired memory, itching/tingling of face, redness of skin, and warmth around the ear (Table S1). All symptoms were asked participants to answer yes or no in the questionnaire (Have you ever been experienced symptoms below during or after using the mobile phone?).
Statistical Analyses
To test the difference of frequencies of mobile phone own by age, gender, and other factors, we used Chi-square test. The t-test or ANOVA were used for tests on the mean ages of first own mobile phone by gender or school grades, and monthly fee for mobile phone use by individual or community level SEP. The multivariate logistic regression was performed to estimate the risk of subjective symptoms for using mobile phone. All analyses were done using the SAS version 9.0 (SAS Inc., Cary, NC, USA) with a significance level of 0.05.
Results
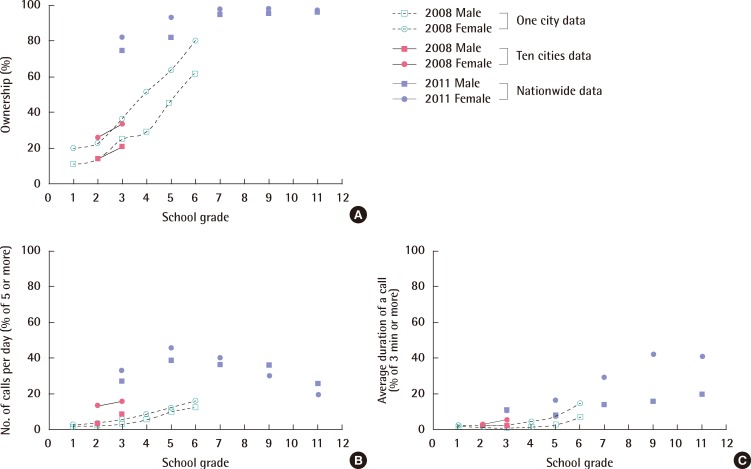
The rate of mobile phone ownership was significantly higher in females than males and increased with children's school grade. The number of calls per day and average duration per call, which represent the amount of mobile phone use, also increased with children's school grade, and was generally higher in females than males throughout all grades. The rate of ownership was markedly increased with time, i.e., 25.2 to 20.9% in 3rd grade elementary school students in 2008 to 74.6% in 2011. More than 90% of 5th grade elementary school students had mobile phones in 2011 (Figure 1).
Average age to own first a mobile phone was 10.4 years. Females tended to have their initial mobile phone earlier than males, and the initial age at which children acquire their mobile phone decreased with time, i.e., younger in current elementary school students and older in current high school students (Table 2).
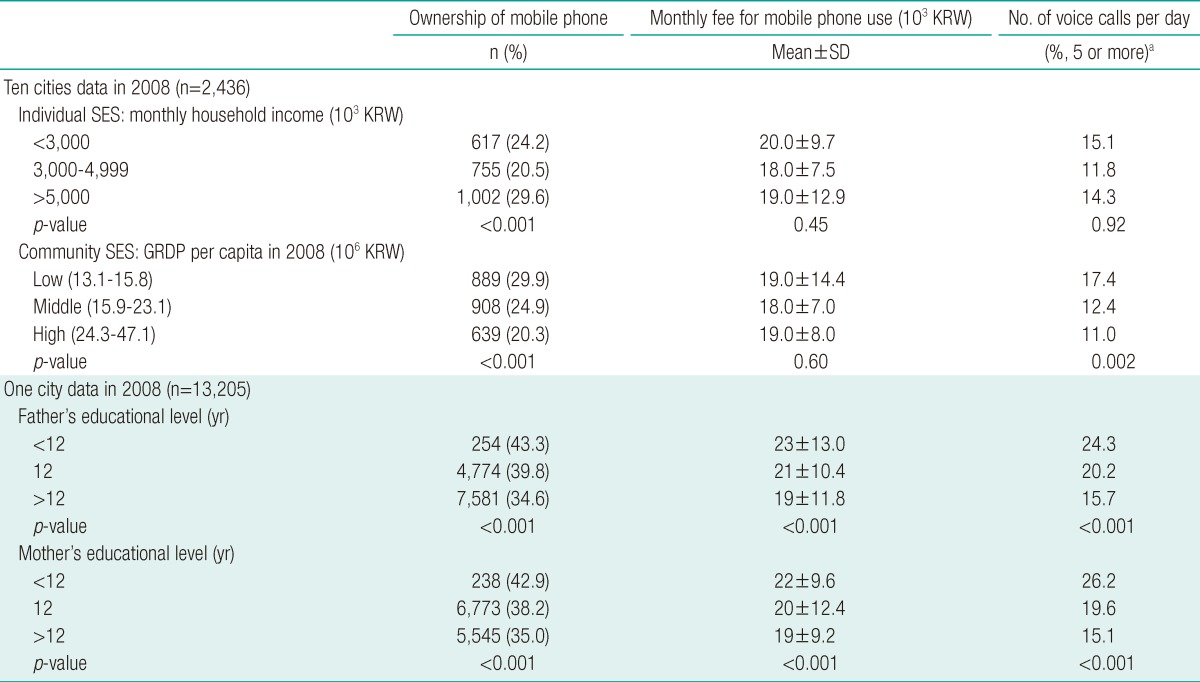
The ownership rate of mobile phone was the highest in the highest individual socioeconomic status (SES) group while it decreased according to the increase of community SES level. The number of calls per day was the highest in the lowest community SES group. The ownership rate, monthly fee for mobile phone use, and the number of calls per day significantly decreased according to the increase of educational level of either parents (Table 3).
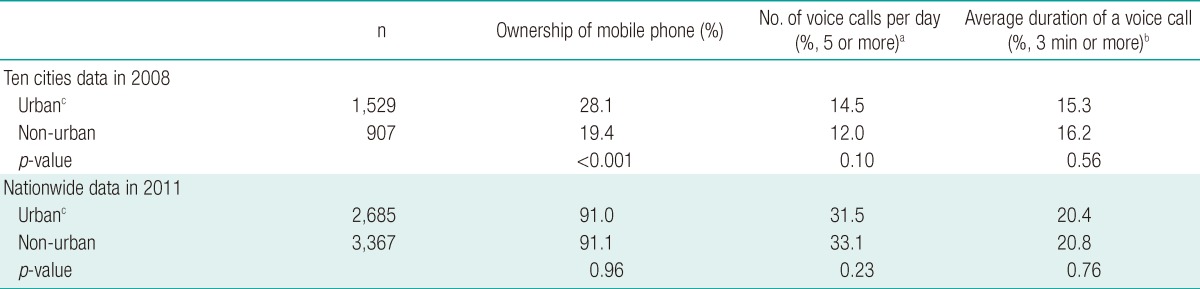
The rate of ownership of mobile phones in 2008 was higher in children living in urban areas compared to those in rural areas. However, there was no difference in the number of calls per day or average duration per call between the two types of areas. In the 2011 nationwide data, there was no difference in mobile phone ownership or in the amount of between urban and non-urban areas (Table 4).
Health symptoms, such as feeling of discomfort and dry skin were associated with the number of outgoing calls per day. Dizziness, dry skin and fatigue were associated with average duration per call. Impaired concentration and impaired memory were associated with all three categories, the number of outgoing calls per day, average duration per call and cumulative time spent on voice calls (Table S1).
Discussion
The ownership rate of mobile phones in Korean children and adolescents has been rapidly increased from 2008 to 2011 and was higher in females than males, which was consistent with previous studies [6,7], although other studies showed different results [8]. Females are more sociable, talkative, and stress greater importance on communication in relationships than males, which may have led them to be more likely to own mobile phones [9]. Greater security concerns parents have for their daughters may be another explanation for the high rate of mobile phone ownership in females [10], which may also explain why females tend to acquire a mobile phone at an earlier age than males.
The ownership rate of mobile phones increased with age, which was also seen in previous studies [8]. The need for children to acquire a mobile phone may increase with age as more activities start to take place outside of home and as their peer groups expand [10]. Parents may also feel the need to buy mobile phones for their growing children for security and emergency reasons [9]. It is noted that mobile phones play an important role in developing peer groups in children [11]. Children persuade parents to buy them mobile phones, especially as peer groups start to play an important role in their lives. A previous study has also discussed about the possible role of mobile phones as a symbol of independence for one of the reasons that drive growing children to acquire a mobile phone [12]. However, given that these pervious papers were written when mobile phone technology was fairly new to the society, it would not be fully appropriate to apply such suggestions to the current findings because mobile phones are very commonly used throughout the society today.
Females generally spent more time on their mobile phones than males over all age groups, with a greater number of calls per day and a longer average time per call, which are consistent with results from previous studies [7,9,13,14]. These results may corroborate the possible existence of traditional gender role within the mobile culture, with females showing more interest towards the interactive side of communication technology, rather than the innovative counterparts [10]. Furthermore, along with the higher ownership of mobile phones, the results may again be reflecting the importance females place on communication in relationships and their greater communicative capacity. A Japanese study [15] which examined different predictors for problematic mobile phone use suggested that high use of mobile phones in females living in Asian countries may be influenced by their conservative cultural background in which talking on the phone may be one of the conventionally accepted ways of alleviating stress obtained from the high level of social pressure burdened upon women.
The mean age at which children acquire their initial mobile phone has dropped significantly over time, with current elementary students acquiring their first phone about an average of 4 years earlier than current high school students. It has been reported that younger people, compared to the old, have more problems associated with excessive use of mobile phones because of their ability to embrace new technology faster [16]. Although the age group of the study's subjects ranged from 18 to 80, which is far wider than that of the present study, it still suggests the possibility of increased problems related with mobile phone addiction in the future generation, as there is a tendency for children to acquire a mobile phone at a younger age.
It was surprising to find higher ownership of mobile phones and amount of mobile phone use in communities with lower SES levels. Similar results, however, have been documented in a German study in which a higher proportion of mobile phone owners and users were found in classes with more families with lower SES [17]. On top of exploring the associations between SES and mobile phone use at a community level like previous studies, the present study also explored the associations at an individual level. The results showed a higher level of mobile phone ownership in higher individual SES groups. As contradictory as these results may seem, they may be supporting previous suggestions that mobile phones may still be viewed as a status symbol and a symbol for compensating social deficits [8,18]. The higher percentage of mobile phone owners in lower SES communities may also be the result of more parents buying mobile phones for their children for safety reasons in these respective areas [19].
Parents' education level was also found to be one of the factors related with children's mobile phone use, with a higher proportion of mobile phone owners and intensive users in children with parents of lower education level. Studies showing similar results have been reported [17,20], and offered a possible explanation that parents with lower SES could be less concerned about possible adverse health effects of mobile phones, thus, not monitoring their children's use of mobile phones as much as those in higher SES groups. On the other hand, parental educational level also represents the individual SES at least in part. However, due to the lack of data availability, we could not explore the similarity in two possible indices for individual SES using a same dataset, i.e., household income and parental educational level.
The rate of phone ownership was higher in children living in urban areas than rural areas in 2008. Most Korean children living in urban areas are often subjected to go to different academic schools after regular school hours to get ahead in their fierce academic race. Therefore, more parents in urban areas may buy their children mobile phones to monitor them for their children's daily schedule, and also for security reasons as some of these academic schools tend to end late at night. On the contrary, the academic environment is much more lenient in rural areas compared to urban areas, which may explain the difference in mobile phone ownership between these two groups. However, the amount of mobile phone use did not differ between the two groups. This may indicate that children in urban areas may own more mobile phones but lack the time to use them compared with children in rural areas, either for socialization or entertainment, due to the greater amount of academic study. A previous study from Spain [9] showed that children living in rural areas actually used their phone more intensively. It was suggested that children may be compensating the feeling of isolation due to transportation difficulties and the limited offer of cultural activities in rural areas by using mobile phones [21]. However, this may not be the case in Korea, as Korea is a more densely populated country than the countries these previous studies were based on. Therefore, with shorter physical distance between rural and urban areas and a well established transportation system, Korean children living in rural areas may not feel as culturally or socially isolated from those in urban areas, ultimately not having to turn to their mobile phones as a source of consolation. No difference between the two regions, urban versus non-urban, in 2011, in terms of ownership or amount of use of mobile phone, may be interpreted at least in part due to the closely connected Korean society regardless of regional areas.
A number of health symptoms seemed to have been aroused in children by more intensive use of mobile phones, especially those related with children's concentration and memory. Similar symptoms and health complaints including headaches and fatigue after using mobile phones have been reported in previous studies [13,22]. Various studies have suggested radiofrequency (RF) emitted from mobile phones as one of the possible causes of these symptoms, however, recent studies have documented no association between these two factors [23]. It has been suggested that the effect of heat or noise from mobile phone use [24] or the nocebo effect may be the possible cause [23,25-27] for these health symptoms. Nonetheless, with the lack of studies regarding the effect of accumulated exposure to radiofrequency in children, and no solid conclusion over the question of whether children are more susceptible to the exposure of radiofrequency waves [28,29], it is still advised that children take precautionary measures to avoid unnecessary exposure to mobile phones [19]. According to increase use of smart phone, it can be expected to see somewhat different pattern of health symptoms because of lengthening mobile phone use time, particularly use for social network system.
Besides the possible adverse effects due to RF exposure from mobile phones, several other problems can arise in the future with growing number of children using mobile phones. Development of information and communication technology, including mobile phones, have provided a fertile ground for cyberbullying [30]. Mobile phones also provide an easier access to violent games and provocative videos for children. This may cause a problem with normal development of children's character, as numerous studies have already shown significant associations between exposure to violent media and aggressiveness in children [31]. Owning a mobile phone or an intensive use of it have also been reported to be associated with health compromising behaviors in adolescents, such as smoking or drinking alcohol [32,33]. Moreover, there are concerns of the role of mobile phones in assisting peer-group bonding in expense of family orientation [11], which may lead to serious social dilemmas, especially, in a family-oriented country like Korea.
There were several limitations to this study. The three databases that were used in this study were not representatively sampled data. Furthermore, there were some differences from whom the information was acquired for each data. For example, the information for the nationwide data was based on self-reported questionnaires answered by children while the other 2 datasets were collected from children's parents or guardians. Previous studies have reported that a difference exists between the actual and the self-reported use of mobile phones [34], which may have lead to a misclassification bias in the amount of mobile phone use.
To prevent unnecessary exposure to RF from mobile phones and social or developmental adverse consequences from excessive use of mobile phones, precautionary measures regarding the use of mobile phones for children and adolescents are needed.